

Selection process
The study selection process is illustrated in the PRISMA-ScR flow diagram (see Fig. 1). A total of 360 records were identified through comprehensive database searches. After the removal of duplicates, 223 records remained and were screened by two independent reviewers based on titles and abstracts using CADIMA software. Discrepancies between reviewers were resolved through discussion and consensus. Following this initial screening, 125 records were excluded for not meeting the inclusion criteria. The remaining 98 articles underwent full-text review. Of these, 77 articles were excluded—21 due to the unavailability of full texts and 56 for not meeting the eligibility criteria. Consequently, 21 studies were included in the final synthesis. Efforts were made to retrieve full texts of inaccessible articles by contacting corresponding authors, searching institutional repositories, and utilizing interlibrary loan services. Despite these efforts, some articles could not be accessed due to unresponsive authors or lack of publicly available copies. This limitation may have led to the exclusion of potentially relevant studies.
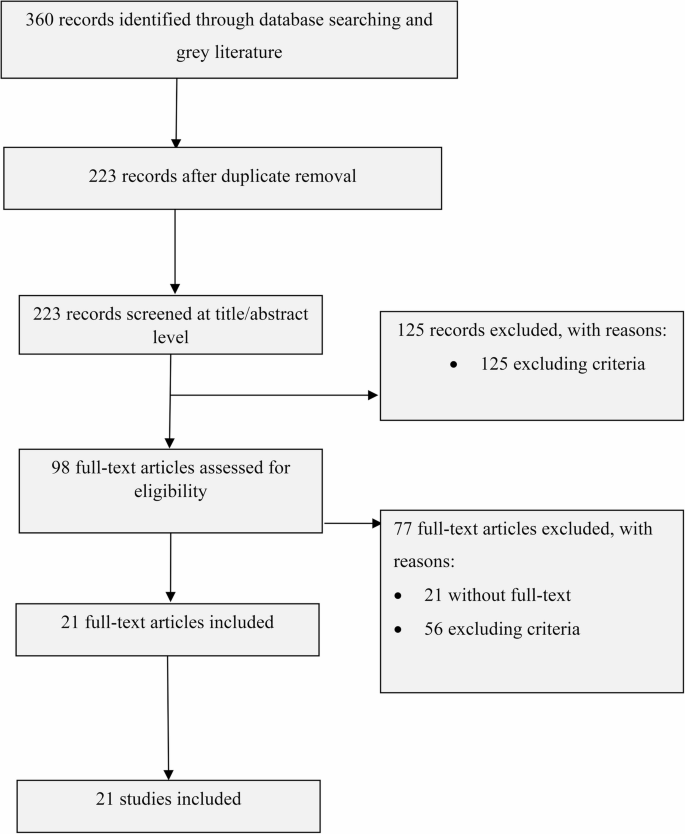
Reporting items for systematic reviews and meta-analysis (PRISMA-Scr) flow chart
Characteristics of the included studies
The 21 included studies cover the period from the inception date of the database to July 2024, and span five different countries (Ethiopia, South Africa, Nigeria, Angola, and Kenya) within the sub-Saharan region. A majority of the studies (n = 14) were based in South Africa with the other countries being Nigeria, Angola, Ethiopia and Kenya. The studies used a variety of study designs, inclusive of qualitative case study methodologies, phenomenological approaches, and interpretative phenomenological analysis (IPA) to explore various aspects of QoL among older people in care facilities across different African countries.
Key data collection tools included in-depth interviews, storytelling, observation checklists, and semi-structured interviews. Several validated questionnaires were also employed, such as the World Health Organization Quality of Life (WHOQoL) questionnaire, WHOQOL-OLD (an Older people WHOQOL module), the Satisfaction with Life Scale, and the Perceived Health Scale. Additionally, the Six-Dimensional EuroQol questionnaire (EQ-6D) and the ICEpop capability measure for older people (ICECAP-O) were used for assessing QoL. The studies also made use of the WHO (Five) Wellbeing Index (WHO-5), Kessler-6 (K6), and OSLO-3 Social Support Scale, along with the Ryff’s Psychological Well-being Scale (RPWBS), the University of California Loneliness Scale (UCLA-LS), and the RAND 36-Item Health Survey. Structured questionnaires captured personal information, physical activity, and attitudes, while other tools, such as the Life Satisfaction Index A, Likert Scale questionnaires, and productivity and generativity indicators, were also applied.
Out of the total (N = 21), majority of the studies (n = 10) were conducted in privately funded LTC facilities (see Fig. 2 below). The majority of participants in these studies were older females, above 65 years of age. Ethnic diversity was a critical factor, with some studies conducted in South Africa focusing on predominantly White participants [48, 49], while others include a significant proportion of Black South Africans or other ethnic groups [50, 51]. In addition to gender and ethnicity, socio-economic status and educational background influenced the findings. Some studies, such as Odetola et al. [52], focus on more affluent populations in well-established geriatric homes, while others explore populations in lower socio-economic conditions or publicly funded institutions, as in Chipps and Jarvis [53] and Teka and Adamek [54]. The variation in these factors related to issues of access to care, social capital, and overall well-being.

There were three main topic areas in the included studies. First, there were studies that describe or develop specific QoL models or scales for older people living in LTC. Secondly, there were studies that qualitatively explore perceptions of QoL both from stakeholders and older people. Lastly, there were studies that examine the relationships between QoL factors, some of which may serve as predictors of QoL. Four key interconnected themes related to the QoL of older people in LTC facilities were synthesized and categorized using Bronfenbrenner’s ecological systems theory, including (1) microsystem, (2) mesosystem, (3) exosystem, and (4) macrosystem (Table 4).
Findings across ecological system levels
Bronfenbrenner’s ecological systems theory was employed as a conceptual and analytical framework to interpret the data rather than as a tool for data collection. The theory provided a structured lens through which to examine how different environmental systems—ranging from immediate interpersonal relationships (microsystem) to broader socio-political structures (macrosystem)—interact to influence the quality of life of older people in long-term care facilities. This theoretical framing guided the organization and analysis of findings by helping to identify the multilevel factors and interactions that shape institutional practices and residents’ everyday experiences (see Table 5 for a summary of findings).
Microsystems
The microsystem is the innermost layer of Bronfenbrenner’s ecological theory and consists of direct interactions between the individual and their immediate environment. The study conducted by Chipps and Jarvis [53] reveals that older people in residential care experience diminished social capital, which subsequently affects their mental well-being. The separation from significant others and limited interaction with external communities contribute to feelings of social isolation among older people [50, 55,56,57]. These studies show that relationships could either foster social bonds or exacerbate isolation, depending on the quality of the relationships and participation in group activities within the facility. Those with higher involvement in activities, both inside and outside the facility, have shown better mental well-being [49, 58]. However, low participation in external activities, as noted by Chipps and Jarvis [53], suggests a barrier within the microsystem, which limits opportunities for older people to engage and improve their QoL.
The caregiver’s role within the microsystem is crucial for the older people’ emotional and physical well-being. Stuart-Röhm et al. [59] emphasize the importance of person-centered caregiving, which focuses on recognizing the individual’s uniqueness and meeting their emotional needs. When caregivers engage in meaningful interactions, such as person-centered caregiving through activities such as singing, the mood and cognitive function of the residents improve, thus creating a more supportive microsystem. For example, the paper by Govender and de Jongh [55] highlights how facilitated communication among older people with hearing impairments by caregivers significantly improved the participants’ QoL. In another study conducted in Kenya, older people reported positive impact on their QoL following care given by both care workers and family members who volunteered at the LTC facility [60].
The physical environment of the facility directly influences interactions in the microsystem. Teka and Adamek [54] highlight the lack of basic amenities, such as soap and toilet tissue, in some residential care centers, as negatively affecting the psychosocial well-being of the residents. Other studies highlight repetitive food and inadequate health services as generating dissatisfaction and creating a hostile microsystem where residents feel neglected [51, 54]. Additionally, the restrictive nature of LTC homes similarly made older people feel dissatisfied because they lack the needed privacy and autonomy [51]. Gerber et al. [61] and Kago et al. [60] show that having a private room enhances the older person’s sense of privacy and dignity.
Mesosystem
The mesosystem in Bronfenbrenner’s ecological model refers to the interactions between different parts of a person’s microsystem. In the context of older residents in LTC facilities, it involves the dynamics between residents, their families, caregivers, and institutional support structures. These interactions play a crucial role in shaping the residents’ overall QoL, mental well-being, and social capital.
Several studies in this review highlight the importance of family relationships to the well-being of older people [51, 52, 54, 57]. Teka and Adamek [54] emphasize that meaningful interaction with family is central to promoting QoL in older residents. As such, many residents express a desire for more frequent contact with family members, which is often restricted in institutional settings [62,63,64]. As Ntozini and Abdullahi [50] put it, the identified lack of family interaction contributes to feelings of loneliness which negatively affect the psychological well-being of residents. Gutiérrez et al. [56] and Odetola et al. [52] emphasize the decline in life satisfaction among older people in LTC facilities, especially those with poorer health or lacking family ties.
The concept of social capital is crucial in understanding the mesosystem. Chipps and Jarvis [53] discuss how residents in LTC facilities often experience diminished social capital due to separation from their families and community. Social capital, which refers to the resources and support derived from social networks, is significantly linked to residents’ mental well-being [65]. When residents are disconnected from their families or community networks, their sense of support and belonging decreases, leading to decreased well-being [50, 52, 58, 66]. The support structures provided within the LTC facility itself, such as caregiver relationships and organized social activities, attempt to mitigate this loss [54]. This is evidenced by Pienaar et al. [49] who found that caregivers play an essential role in fostering residents’ physical and mental health by encouraging physical activities. The quality of the relationship between residents and caregivers serves as another key component of the mesosystem which directly impacts the residents’ QoL and mental health.
Stuart-Röhm et al. [59] focus on the person-centered care approach, which involves caregivers recognizing residents’ individuality and emotional needs. This approach improves the relationship between residents and caregivers, enhancing mutual well-being and creating a more nurturing environment. Caregivers also influence the residents’ level of engagement in activities that promote social connections. A well-functioning mesosystem requires effective communication between caregivers and the residents’ families. Govender and de Jongh [55] highlight that residents with hearing impairments often face social isolation, but when caregivers actively support their use of hearing aids, social interactions and QoL improve. Similarly, caregivers in Hanssen and Kuven’s [51] study brought traditional foods from home to improve the social and emotional well-being of residents, demonstrating the deep emotional connections that can develop between residents and caregivers in an institution. Kago et al. [60] found that emotional and financial support from families, when combined with high-quality care from the institution, contributed positively to the psychosocial well-being of elderly residents. Families and caregivers must collaborate to provide holistic care, yet this analysis suggests that such cooperation is often lacking. Many families have limited involvement, placing a greater burden on caregivers, which can negatively affect the residents’ psychosocial environment.
Exosystem
Several studies in the analysis indicate the significant influence of enabling institutional policies on the QoL of elderly residents. Kago et al. [60] highlight the direct impact of institutional policy frameworks on the psychosocial well-being of elderly individuals. For instance, policies that provide emotional support, home repairs, financial support, and social services can significantly improve residents’ lives. This aligns with Bronfenbrenner’s concept of the exosystem, where policies outside the individual’s immediate environment (i.e., management frameworks) shape their lived experience. Ntozini and Abdullahi [50] and Hanssen and Kuven [51] emphasize the need for policies that address cultural diversity within LTC homes. The South African philosophy of Ubuntu, which focuses on communal care and interconnectedness, was proposed by Jarvis et al. [56] as a model to combat isolation. Stuart-Röhm et al. [59] emphasize the importance of person-centered care within LTC facilities, particularly for residents with dementia. The study advocates for frameworks that recognize individuality and aim to enhance emotional and social needs. Oluwagbemiga [67] adds that well-structured support systems, including emotional and informational support, and companionship, are essential in improving psychological well-being in LTC. The importance of caregiver training and its influence on the well-being of residents is evident. Kago et al. [60] and Oluwagbemiga [67] stress that caregivers need specialized training in gerontology and mental health to meet the psychological and social needs of the elderly. This reflects Bronfenbrenner’s notion that institutional training programs, though indirectly related to residents, have a profound impact on the quality of care they receive. Odetola et al. [52] concur by recommending the inclusion of geriatric care in nursing and health professional curricula to improve the overall care framework in LTC facilities. Further, Teka and Adamek [54] call for better training of healthcare workers in geriatric care, more flexible policies, and family-friendly environments to enhance life satisfaction of LTC residents.
Macrosystem
The macrosystem includes broad societal factors, such as cultural norms, economic conditions, and public policies that influence individual and group behaviors. The WHOQOL-OLD instrument, referred to across studies, reflects an international effort to assess QoL among older people [16, 55]. However, the cultural fit of these tools, as suggested by Van Biljon and Roos [26], and in further work conducted by Van Biljon et al. [16], raises concerns. In South Africa, validation in the mother tongue is recommended to better address the cultural relevance for local populations. Cultural differences also emerge regarding food preferences and psychosocial health [54]. Hanssen and Kuven [51] note that traditional food plays a critical role in the well-being of dementia patients in South African LTC facilities. The incompatibility between the food provided and cultural preferences significantly affect emotional and social well-being [51, 54]. The societal perception of aging in sub-Saharan Africa is marked by vulnerabilities, such as poverty, exclusion from health services, and insufficient family support systems [56, 58]. Institutional care appears to carry different meanings across racial and economic divides in South Africa. Ramocha et al. [58] observed that White older persons often enter institutional care with better financial planning, whereas Black older South Africans do so out of destitution. This stark difference suggests that societal views on aging and care are deeply influenced by socio-economic conditions. Govender and de Jongh [55] further emphasize the stigma associated with conditions such as hearing loss, which can lead to social isolation.
Guided by Bronfenbrenner’s ecological systems theory, the discussion of findings reflects a multilevel understanding of the quality of life of older people in long-term care. The theory enabled us to map how experiences at the individual and interpersonal levels are influenced by institutional policies, community dynamics, and broader structural conditions. This ecological perspective emphasized the interconnectedness of systems and underscored the importance of addressing not only immediate care practices but also systemic factors such as governance, staffing norms, and social policy.
link