



The GQC meets monthly with the overarching goal of improving and monitoring the quality of care for hospitalized older adults. Before the meeting, an agenda with targeted focus areas is prepared, and the council, chaired by the Geriatric Division Chief, reviews and discusses those topics.
The GQC is responsible for selecting and defining quality metrics and setting effective goals for each metric. Baseline data collected initially before implementing the intervention is considered the control for each metric, and a quality improvement plan is created to meet the pre-set goals. The plan, at a broader level, includes educating all care team personnel, creating or optimizing workflows, and utilizing electronic health record functionalities. In addition to the educational materials, focused care plans are created based on the selected metrics.
The Quality Improvement Advisor and the HELP Elder Life Specialist provided administrative support for the GQC by scheduling the monthly meetings, setting the agenda, and monitoring implementation. The HELP Elder Life Specialist and the hospital’s digital technology services (DTS) extracted data. Data analysis and reports were prepared by the Quality Improvement Advisor and the HELP Elder Life Specialist.
The real-time monitoring system tracks intervention implementation. A daily chart review of the selected sample is done for all metrics. If deviations are observed, feedback is provided to appropriate team members immediately. Data collection is a combination of manual data extraction and EHR reports. Some of the data is monitored daily through other quality improvement processes like the indwelling catheter days. Monthly data for each individual metric is compiled and presented for GQC review to identify any gaps in care, and feedback from interdisciplinary teams is received. Specific quality improvement interventions are developed to address these gaps. Appendix Table 1 and Fig. 5. show details and the timeline of the metrics and relevant interventions. After the discussion, possible evidence-based solutions are brainstormed, appropriate action items are created and assigned to the concerned individual/department, and progress is monitored.
Data management
Data is collected for a random sample of 20–40 patients monthly. The model uses the baseline data collected for each metric as control data before implementing quality improvement interventions. Thereafter, monthly data is analyzed and presented in percentages to monitor improvement trends (Appendix Table 2). The design is similar to the longitudinal design, collecting repeated measurements of each metric.
Data sources include electronic health record (EHR) chart reviews, administrative reports from the Business Intelligence Department [9] (Hospital digital technology services that help run the automated data extraction utilizing electronic health records), and data collected for HELP.
Data trends
Data from all sources was pooled to form one comprehensive dataset. This was used to monitor data trends. The preset goal for each metric was the reference point to map improvement in the metric. Data fluctuation was anticipated as the initiatives for the metrics were administered in PDSA cycles. The graphs found in Appendix Fig. 4 show the fluctuations in data. Factors such as staffing, new hires, changes in quality improvement initiatives across the hospitals, COVID-19 pandemic and the complexity of the patient’s condition contributed to these fluctuations.
Intervention feasibility, dissemination and real-time monitoring system
All interventions before implementation are assessed for feasibility with interdisciplinary teams involved in the planning stage. Possible barriers to implementation are uncovered, and solutions are brainstormed collectively in the GQC meeting. The dissemination process includes nursing and clinician education, creating specific workflows, such as nursing-driven catheter protocol, optimizing EHR workflows like flowsheets for hearing impairment, real-time chart reviews, and one-on-one education. The HELP Elder Life Specialist plays an important role in disseminating and monitoring the implementation.
The time series design of the model enables the GQC to track real-time implementation trends. The comprehensive dataset at the patient, unit, and certain service line levels (GED) allowed for source identification and prompt intervention for a particular metric. Timely changes are made to the intervention to overcome barriers and meet the goal. This process continues until the intervention is fully implemented and target goals are reached and sustained. Active tracking of the intervention implementation is continued unless other quality improvement projects monitor data for the same metrics (for example, 30-day readmission data).
Step-by-step integration: evolution of the care model

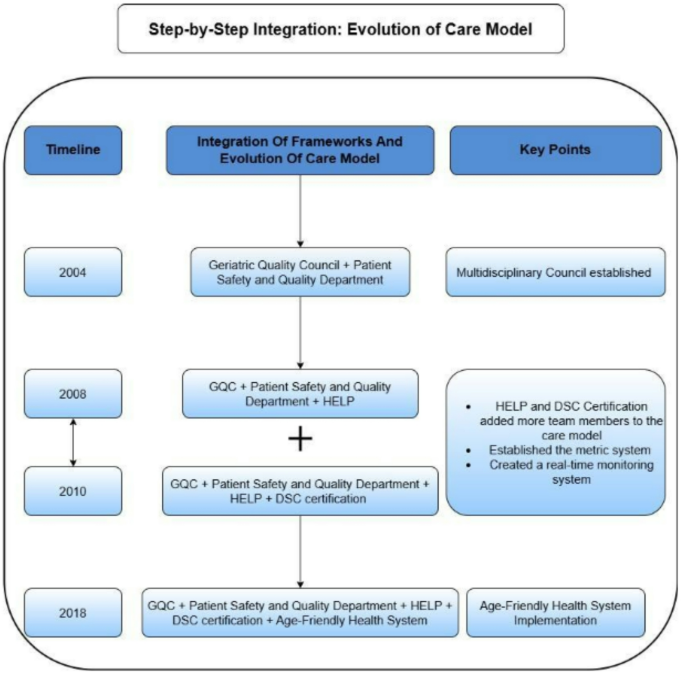
This diagram describes the timeline of integration of multiple geriatrics friendly frameworks in the Interdisciplinary Care Model
The integrated framework evolved from a series of quality improvement projects undertaken to reduce the hazards of hospitalization for older adults at HUMC (Fig. 2). The Geriatric Division at HUMC established the Geriatric Quality Council in 2004. The newly formed Quality Council was an interdisciplinary team with members from various disciplines, such as geriatricians, nursing staff, physical therapy, speech therapy, dieticians, case managers, pharmacy, and social workers. The aim of the council was to monitor the quality of care for hospitalized older adults and its effect on health outcomes. The GQC meets every month, discusses the monthly agenda, and follows up with actionable items.
In 2008, the Hospital Elder Life Program (HELP) was incorporated into the care model to manage cognitive decline in older adults in a hospital setting. This provided additional team members, such as the HELP Elder Life Specialist and volunteers. The HELP program enabled us to build on evidence-based interventions, with access to trained volunteers, a valuable resource for delirium prevention. Along with integrating the HELP Framework, the quality council created a real-time monitoring system that allows timely intervention or implementation changes to achieve the set goal. The system initially started tracking the data collected from the HELP patients and later extended it to all hospitalized older adults. The HELP Elder Life Specialist collected and monitored data daily. This was presented as a monthly report to the GQC for review and discussion.
The data management and real-time monitoring system incorporated into the care model paved the way for more achievements. In 2010, HUMC started the first geriatric delirium DSC certification process to address delirium. Incorporating the certification process was also a strategic move to gain executive support and resources. It embedded education as an important intervention. The certification process requires selecting valid, reliable performance measures relevant to the target population based on clinical practice guidelines or other evidence-based practices. For the application, four clinical performance metrics impacting the care of hospitalized older adults are selected using the gold standard guidelines and literature reviews. A new metric is selected once a particular metric consistently performs at the pre-selected goal. This process added the additional step of monitoring the quality metrics of the care model, perfecting the existing system, regulatory oversight, and ensuring consistency in high-quality care delivery. We were first certified as a geriatrics delirium program by the Joint Commission in 2011.
The well-established care model with various EHR optimizations facilitated HUMC’s enrollment in the Age-Friendly Health System model in 2018.
link